Introduction
The cervical-cranial-facial postural system enables three-dimensional movement and breathing through balanced neuromuscular function. Its development is shaped by anatomical and physiological factors, including tongue posture relative to the palate, craniofacial structure and sensory-motor behaviors that both influence and are influenced by their anatomical framework. Nutritional status, interacting with epigenetic mechanisms, is another major factor guiding craniofacial growth and function. This article explores how postural, developmental and nutritional elements interconnect and identifies potential intervention points to restore or maintain optimal cervical-cranial-facial structure and function.
Connecting Postural Dysfunction and Craniofacial Development
Tongue Posture and Nasal Breathing
Habitually posturing the tongue on the palate has significant benefits for postural and craniofacial function. Provided there is sufficient nasopharyngeal space, this posture promotes nasal rather than mouth breathing. Nasal breathing warms, humidifies and filters inhaled air, optimizing gas exchange. It also stimulates nitric oxide production in the sinuses, which promotes lung vasodilation and acts as a potent antibacterial and antiviral agent.
In contrast, mouth breathing lowers and retrudes the tongue, mandible and hyoid. This can partially occlude the oropharyngeal airway, leading to compensatory posterior cranial rotation to maintain airway patency. To level the ocular plane during compensatory upper cervical and cranial extension, the neck adopts a forward and flattened cervical lordosis (Solow et al, 1993).
Mandibular and tongue retrusion moves the hyoid downward and backwards, further exacerbating airway narrowing. Forward head posture attempts to compensate for this by repositioning the hyoid in an attempt to increase airway patency (Meiyappan et al, 2015). However, forward head posture also tends to lengthen and narrow the airway, increasing susceptibility to collapse and apnea behaviors (Yeol et al, 2013). The system struggles to maintain balance.
Mouth breathing is also associated with increased accessory muscle breathing, shoulder and pelvic asymmetries and reduced nocturnal activity in key airway dilators such as the genioglossus, tensor palatine, upper airway dilators and intercostals (Uhlig et al, 2015).

Functional Parallel Between the Diaphragm and Tongue
The diaphragm and tongue share functional similarities. The diaphragm pumps air and lymphatic fluids through oscillatory downward contraction during inhalation and elevation during exhalation (relaxation), with a pause before the next breath. When the diaphragm reaches its highest point during exhalation, it is maximally opposed to the rib cage—a region known as the zone of apposition.
The Postural Restoration Institute emphasizes the importance of the zone of apposition in restoring correct breathing and postural function (“Postural Restoration Institute,” 2013). A poorly opposed diaphragm may remain contracted and downward, leaving an individual in a chronically inhaled state of being. This tension can extend to the tongue above and the psoas below due to anatomical connections, contributing to lumbar lordosis, anterior-inferior rib cage elevation (external rotation) and numerous compensatory postural adaptations throughout the body.

Swallowing Mechanics Act as a Cranial Pump
Swallowing complements respiratory phases, helping to pump fluids and air.
During a swallow, the tongue moves in a wave-like motion from anterior to posterior across the palate. Frequency of swallowing varies widely depending on salivary flow and volume, ranging from 18–400 times per hour (Rudney et al, 1995). The Academy of Orofacial Myofunctional Therapy cites 500–1000 swallows per day for humans, while Orofacialmyology.com reports adults swallow roughly 585 times per day and children 800–1000 times per day.
Swallowing generates upward force against the palate. McGlone and Proffit (1973) measured this as 150–200 g/cm² (≈1 lb/in²), though other sources suggest up to 4 lbs. Regardless of the exact number, this rhythmic pressure on the maxilla and sphenoid facilitates cranial flexion and extension, potentially aiding cerebrospinal fluid movement. For this reason, the tongue is often described as the cranial diaphragm, “pumping” the cranium.

Braking Effect of the Tongue on the Palate
Tongue-on-palate posture provides a stabilizing “brake” for the cranial system, countering asymmetrical neuromuscular torque. The right diaphragm is naturally thicker, with broader spinal attachments and greater strength than the left. This asymmetry tends to orient the lower thoracic and upper lumbar spine (T8–L3) to the right.
To maintain forward orientation, the spinal segments above T8 often rotate left, increasing anterior flaring and external rotation of the lower left ribs. This torsional force ascends through the postural chain, influencing craniofacial structures. Research shows nearly 75% of cranial strain patterns involve an elevated right sphenoid, reflecting this common right-sided dominance (Timoshkin et al, 2008).
The left diaphragm leaflet often has a reduced zone of apposition compared to the right. Restoring left-sided apposition reduces torsional strain through the postural system. Likewise, maintaining even tongue contact on the palate anchors the maxilla, stabilizing cranial structures and reducing the risk of postural and craniofacial asymmetry.
Cranial Zone of Apposition
A cranial zone of apposition of the tongue against the palate exerts consistent expansion forces on the maxilla, helping maintain dental arch size and prevent malocclusion. Without this opposing force, the arch can be overwhelmed by the constrictive activity of the orbicularis oris, buccinator and mentalis muscles.

Dynamic Neuromuscular Balance
The orbicularis oris, buccinator and superior pharyngeal constrictor form a neuromuscular sling surrounding the dental arch and airway. This sling continues via the middle and inferior pharyngeal constrictors around the airway. Over-activation of this chain can constrict both the dental arch and airway, emphasizing the importance of balanced tongue-palate function.

Tongue Posture, Swallowing Patterns and Craniofacial Development
A narrow maxillary arch may not provide enough room for the teeth, predisposing to crowding and malocclusion. This can lead to compensatory strain patterns throughout the body (Adhikari et al, 2011). The problem becomes more pronounced when accompanied by a reverse swallow pattern—an anterior tongue thrust—where the tongue pushes forward against the front teeth while the cheeks and lips draw inward through overactivity of the buccinator, orbicularis oris and mentalis muscles.
This infantile swallow pattern originates as a primitive reflex supporting breastfeeding but may fail to integrate into a mature swallow, especially if breastfeeding is not initiated or ends too early. In a normal adult swallow, the tongue moves upward in a wave-like motion against the palate while the facial muscles remain relaxed. In contrast, with a reverse swallow, the tongue pushes forward into the front teeth, which over time can lead to an anterior open bite and increased postural tension.
Often accompanying this pattern, the tongue habitually rests on the lower teeth or between the arches, preventing normal tooth eruption and reducing vertical height. This can further disrupt occlusion and contribute to strain through the craniofacial and cervical regions. Malocclusion is commonly associated with imbalanced cervical, cranial and facial posture and may contribute to temporomandibular joint (TMJ) dysfunction, neck pain and headaches. Ideally, after every swallow the teeth should lightly touch. However, when interferences exist during this contact phase, they can compound postural problems.

Malocclusion with Decreased Vertical Height

Anterior Open Bite

Tongue Thrust
The Role of Tongue-on-Palate Contact
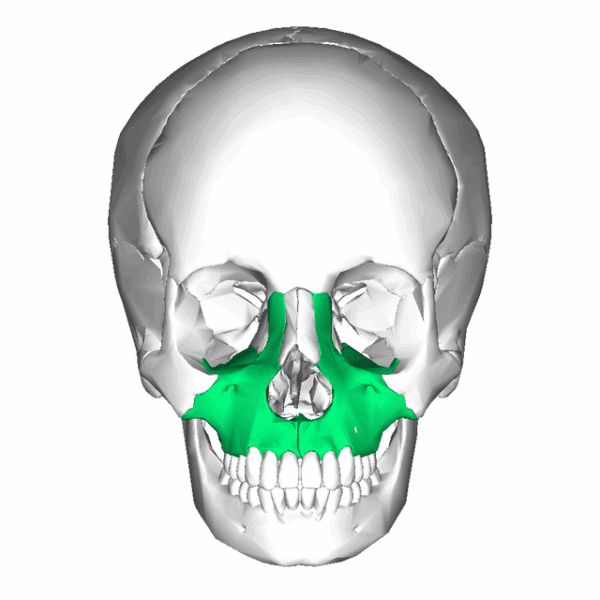
Habitual contact between the tongue and palate guides the growth and development of the craniofacial system. This contact provides a mechanical and cellular stimulus promoting bone growth (Singh et al, 2009). The gentle pressure of the tongue against the maxillary floor encourages forward, upward and outward expansion of the maxilla. Without this stimulus, the maxilla may remain narrow and elongated, setting the stage for restricted airways and altered facial development.


Oromotor Activity and Nervous System Integration
Oromotor activity plays a foundational role in craniofacial development. In utero, the embryo begins forming sensory-motor relationships that coordinate with growth and differentiation. After birth, breastfeeding promotes tongue-on-palate posture and nasal breathing—essential functions for healthy craniofacial and neurological development.
The tongue’s contact with the palate provides a rich neurosensory input that stimulates cranial nerve integration in the brainstem. The vagus nerve, which innervates the palatoglossus muscle, links these craniofacial pathways with autonomic regulation. This cross-communication means activity in cranial nerve nuclei can influence vagal tone and vice versa. Stephen Porges (2011) explains in The Polyvagal Theory that these integrated craniofacial and autonomic systems form the basis for higher cortical functions such as social engagement, executive processing and complex sensory-motor control. Without well-developed cranial nerve regulation, the cortex struggles to integrate primitive reflexes and support advanced functions.

Breathing and Osseous Development
When the maxilla develops inadequately in width or forward projection, the nasal floor becomes restricted, potentially limiting airflow. This may lead to deviated septums, enlarged turbinates or adenoids and turbulent airflow. As nasal breathing becomes more difficult, mouth breathing often takes over, reinforcing dysfunctional postural and craniofacial patterns.
A lack of anterior or lateral maxillary growth reduces dental arch space, leading to crowding and potential Class II or III malocclusions. As previously discussed, these malocclusions are closely tied to postural imbalances.

Deviated Septum
Resting Tongue Position
There is limited research defining the ideal resting tongue position, partly due to challenges in imaging without biasing results. McKee (1956) found that in non-cleft subjects, the tongue apex rested against the lingual surfaces of the lower incisors with the posterior tongue against the soft palate and uvula. In cleft palate individuals, the tongue rested lower. Studies in edentulous patients (Kotsiomiti et al, 2005) also showed the tongue typically resting low in the mouth, which correlated with poorer denture retention. Improved tongue posture, as noted by Lee et al (2009), supports improved oral stability.
The International Association of Facial Growth Guidance (Orthotropics), led by Drs. John and Mike Mew, teaches that the tongue should rest in full contact with the entire palate—both hard and soft portions (Mew, 2013). Clinically, this position tends to correlate with the most balanced craniofacial and postural outcomes. However, if there is significant restriction in the tongue and it is overly strained attempting to achieve this position then it is advised to rest it as high up into the palate as is comfortable without generating increased neck tension.

Tongue Posture Patterns and Ankyloglossia
In practice, the most common pattern observed in individuals with neck, head and jaw tension is little or no tongue-to-palate contact. Often the tongue rests between the arches or only the anterior one-third touches, sometimes pressing against the teeth. Many individuals have never experienced full palatal contact and may lack proprioceptive awareness of this position, often due to tongue restrictions such as ankyloglossia (tongue tie).
Ankyloglossia is an abnormally short, thick, or tight frenulum that restricts tongue mobility. Normally, the frenulum regresses before birth to allow full motion, but when it persists, it can impair breastfeeding, speech and craniofacial development (Rowan-Legg & Society, 2015; Tow et al, 2014). Tongue ties often occur with lip ties and are more common in males.
In addition to a mechanical tongue tie, chronic increased neuromuscular tension stemming below and above the diaphragm when it is not resting in a neutral position can impact the tongue's ability to relax and posture up and around the palate.
Tongue Stretching Technique
If tongue restriction limits full palatal contact, a simple self-applied stretching technique can help:
- Grip: Wrap a small towel, napkin or textured paper around the tongue near its base (close to the frenulum).
- Lift: Gently grip with your fingers, placing thumbs near the frenulum and pull the tongue upward toward the palate, focusing on areas that feel restricted.
- Mobilize: While maintaining tension, open and close your jaw or move it side to side to vary the stretch and engage different fibers.
- Duration: Hold for 1–2 minutes and repeat several times per day. Lying on your back is easiest, but it can also be done seated or standing.
As flexibility improves, practice maintaining tongue contact around the sides of the palate throughout the day—except while eating, drinking or speaking. It can take weeks to reprogram this postural habit, so leaving reminders can help reinforce the new pattern.
As the tongue gain the ability to contact the palate, swallowing can be retrained to ensure that the cranium is receiving adequate pumping along with eliminating any extraneous forces on the front teeth if a tongue thrust exists.
If consistent stretching does not achieve adequate mobility, a frenectomy (surgical release of the tie) may be considered. This is typically performed by a dentist or ENT using laser, scalpel or cryotherapy. However, most cases respond well to conservative stretching and retraining. Tongue tie identification in newborns is especially important since restriction can hinder breastfeeding and early craniofacial development.
Restoring Function and Growth
If the upper dental arch is too narrow to accommodate the tongue, palatal expansion techniques can help restore proper oral space and function. There are numerous options offering different degrees and types of expansion. MARPE (Microscrew Assisted Rapid Palatal Expansion) accomplishes genuine palatal and nasal widening. MMA (Maxillary Mandibular Advancement) surgery elongates the maxilla and mandible surgically.
There are many different kinds of removable palate expanders such as the ALF (Alternative Lightwire Functional Appliance) (Bronson et al, 2015), Orthotropics (Mew, 2013), and the Homeoblock which primarily remodel the alveolar bone to widen the arch. Invisalign and braces also have the potential to open up the arch. As the craniofacial complex expands, nasal and sinus airflow improves, occlusion balances and space for the tongue increases—all supporting more efficient breathing and postural alignment.
In addition to modifying the bony architecture of the dental arch, maxillary expansion appliances apply gentle neurosensory forces across the palate, mimicking the natural pressure of the tongue but with more intensity. For some, this alone can be enough of a stimulus needed to encourage neuromuscular rebalancing in the cervical, cranial and oromotor regions.
Dietary Links to Craniofacial Development
Modern dietary patterns have profoundly affected craniofacial growth and postural health. Over the past 10,000 years and especially within the last century, refined and processed foods have replaced nutrient-dense traditional diets. This shift from whole mineral-rich foods to soft low-nutrient modern fare has contributed to underdeveloped jaws, dental crowding, malocclusion and airway restriction (Boyd, 2011, 2012).
Insights from Weston A. Price
In the early 20th century, dentist and researcher Weston A. Price documented the oral and systemic health of indigenous populations who consumed traditional diets. He observed that communities eating unprocessed locally sourced foods such as wild-caught fish, organ meats, raw dairy and naturally fermented grains and vegetables displayed broad dental arches, straight teeth, robust bone structure and resistance to decay.
When these same populations transitioned to Westernized diets of refined flour, sugar, canned goods and processed fats, Price recorded rapid declines in oral and systemic health within a single generation. Dental crowding, narrow palates, sinus congestion, cavities and susceptibility to infection increased sharply (Price, 2009).
Price concluded that craniofacial and dental health depend more on nutrient density and food quality than on genetics alone. The fat-soluble vitamins A, D and K2 (then termed “Activator X”) played central roles in supporting bone growth, facial development and mineral metabolism. These nutrients, derived from pasture-raised animal fats and seafood, are largely absent in modern industrial diets.


The Legacy of Francis M. Pottenger Jr.
Around the same era, Dr. Francis M. Pottenger Jr. conducted a decade-long series of nutritional studies on more than 900 cats to examine the physiological effects of cooked versus raw food diets (Pottenger, 1945, 2012). Cats consuming a raw diet with unpasteurized milk remained fertile, exhibited strong bone structure, broad facial development and robust immunity. In contrast, those fed cooked or processed food developed skeletal deformities, dental crowding, respiratory issues, allergies and reproductive failure.
Most strikingly, Pottenger observed that nutritional deficiencies compounded over generations. By the third generation, cats fed deficient diets exhibited severe skeletal narrowing, underdeveloped craniofacial structures and infertility. Even when returned to nutrient-dense diets, full recovery was limited, demonstrating that nutritional and structural deficiencies can propagate epigenetically across generations.
Although animal-based, Pottenger’s findings align with Price’s human studies, both highlighting the profound relationship between diet quality, facial structure, fertility and systemic resilience. Together their work underscores the biological cost of processed foods and the regenerative potential of restoring traditional nutrient density.
The Price and Pottenger studies demonstrate that nutrient-dense diets not only influence systemic health but directly support optimal craniofacial growth, jaw width, dental arch development and airway patency.

Nutritional Deficiencies and Craniofacial Development
It has been found that folate influences midline development, tongue ties and cleft palate (Andreou et al., 2007). Folate metabolism also impacts gene regulation, detoxification, neurotransmitter synthesis, hormone processing, DNA synthesis, energy production and cellular health (Lynch, 2012).
When there is reduced folate conversion patterns in the body, bioavailable methylated versions such as L-5-MTHF or L-Methylfolate are recommended along with other nutrients such as the B vitamins as a whole (B-complex).
Environmental factors, digestion, blood sugar regulation, endocrine and immune function, nervous system regulation and toxicity exposure all interact with genetic expression. Prevention and intervention strategies targeting nutrition, early tongue-palate contact and orofacial myofunctional therapy can support optimal growth and function.
Conclusion
Cervical-cranial-facial posture is tightly integrated with tongue-palate mechanics, craniofacial development and sensory-motor function. Ankyloglossia and craniofacial restrictions can negatively impact posture and neuromuscular function. These structural patterns interact with nutrition and the environment. Early prevention, in-utero and postnatal nutritional optimization and targeted intervention strategies—including tongue-palate retraining, orthodontics and maxillary expansion—can improve craniofacial development, posture and overall physiological function throughout life.
What Can You Do to Optimize Your Breathing, Posture and Nutrition?
Applying these concepts begins with awareness of your own body patterns and daily habits. Integrating small yet intentional changes can have profound effects on craniofacial alignment, posture, breathing and overall well-being.
- Ensure you are using your diaphragm correctly.
The diaphragm is central to posture and breathing coordination. We highly recommend techniques from the Postural Restoration Institute (PRI), which emphasize balanced inhalation and exhalation mechanics to restore optimal alignment and respiratory efficiency. - Assess your tongue posture.
Notice where your tongue rests throughout the day. Ideally, it should contact the roof of the mouth with the tip just behind the upper front teeth. Evaluate how you swallow—does your tongue press gently against the palate or do you notice tension in the lips or jaw? Restoring proper tongue posture supports nasal breathing, jaw alignment and craniofacial balance. - Support healthy methylation.
Methylation is a key biochemical process that influences detoxification, energy production and tissue repair. Many individuals benefit from supplementing with high-quality B12 and folate, particularly in active methylated forms. These nutrients are often deficient in modern diets and play an essential role in cellular and neurological health. - Nourish your body with whole foods.
Reflect on the nutrient density of your diet. Emphasize fruits, vegetables, leafy greens and herbs as foundational sources of vitamins, minerals and phytonutrients. When possible, choose local and minimally processed foods that align with the body’s natural design for nourishment and regeneration.
Adhikari, H. D., Kapoor, A. K., Prakash, U., & Srivastava, A. B. (2011). Electromyographic Pattern of Masticatory Muscles in Altered Dention Part II. Journal of Conservative Denstistry, 14(2), 120–127.
Andreou, A. M., Pauws, E., Jones, M. C., Singh, M. K., Bussen, M., Doudney, K., … Stanier, P. (2007). TBX22 Missense Mutations Found in Patients with X-Linked Cleft Palate Affect DNA Binding , Sumoylation , and Transcriptional Repression. The American Journal of Human Genetics, 81(October), 700–712. http://doi.org/10.1086/521033
Boyd, K. L. (2011). Darwinian Dentistry. Journal of American Orthodontic Society, 34–40.
Boyd, K. L. (2012). Darwinian Dentistry Part 2. Journal of American Orthodontic Society, 28–33.
Bronson, J. M., Bronson, J. A., & Holway, C. (2015). Introducing the Advanced Light Force ( ALF ) Appliance. Oral Health, 10–17.
Henderson, G. B. (1990). FOLATE-BINDING PROTEINS. Annual Review of Nutrition, 10, 319–335.
Houghton, L. A., Yang, J., & O’Connor, D. L. (2009). Unmetabolized folic acid and total folate concentrations in breast milk are unaffected by low-dose folate supplements. American Journal of Clinical Nutrition, 89(1), 216–220. http://doi.org/10.3945/ajcn.2008.26564
Kotsiomiti, E., Farmakis, N., & Kapari, D. (2005). Factors related to the resting tongue position among partially and completely edentulous subjects. Journal of Oral Rehabilitation, 32, 397–402.
Lee, J., Chen, J., Lee, H., & Chang, H. (2009). Improved denture retention in patients with retracted tongues. The Journal of the American Dental Association, 140(8), 987–991. http://doi.org/10.14219/jada.archive.2009.0308
Lynch, B. (2012). L-Methylfolate, Methylfolate, 5-MTHF, L-5-MTHF. What is the Difference!? Retrieved from http://mthfr.net/l-methylfolate-methylfolate-5-mthf/2012/04/05/
Mcglone, R. E., & Proffit, W. R. (1973). Patterns of Tongue Contact in Normal and Lisping Speakers. Journal of Speech and Hearing Research, 16, 456–473.
McKee, T. L. (1956). A cephalometric radiographic study of tongue position in individuals with cleft palate deformity.pdf.
Meiyappan, N., Tamizharasi, S., Senthilkumar, K. P., & Janardhanan, K. (2015). Natural Head Position: An Overview. Journal of Pharmacy and BioAllied Sciences, August(Suppl 2), S424–S427.
Mew, J. (2013). The Cause of Malocclusion. Broadfield.
Mitchell, L. E., Murray, J. C., Brien, S. O., & Christensen, K. (2003). Retinoic Acid Receptor Alpha Gene Variants , Multivitamin Use , and Liver Intake as Risk Factors for Oral Clefts : A Population-based Case-Control Study in Denmark , 1991 – 1994. American Journal of Epidemiology, 158(1), 69–76. http://doi.org/10.1093/aje/kwg102
Porges, S. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-regulation.
Postural Restoration Institute. (2013). Retrieved from https://www.posturalrestoration.com/
Pottenger, F. (1945). Effect of Heat-Processed Foods and Metabolized Vitamin D Milk.
Pottenger, F. (2012). Pottenger’s Cats.
Price, W. A. (2009). Nutrition and Physical Degeneration.
Rooij, I. A. L. M. Van, Vermeij-keers, C., Kluijtmans, L. A. J., Ocké, M. C., Zielhuis, G. A., Goorhuis-brouwer, S. M., … Steegers-theunissen, R. P. M. (2003). Does the Interaction between Maternal Folate Intake and the Methylenetetrahydrofolate Reductase Polymorphisms Affect the Risk of Cleft Lip with or without Cleft Palate ? American Journal of Epidemiology, 157(7), 583–591. http://doi.org/10.1093/aje/kwg005
Rowan-legg, A., & Society, C. P. (2015). Ankyloglossia and breastfeeding. Canadian Paediatric Society, 20(4), 209–213.
Rudney, J. D., Ji, Z., & Larson, C. J. (1995). The prediction of saliva swallowing frequency in humans from estimates of salivary flow rate and the volume of saliva swallowed. Archives of Oral Biology, 40(6), 4–6.
Singh, G. D. and Krumholtz, J. (2009). Epigenetic Orthodontics.
Solow, B., Ovesen, J., Nielsen, P. W., Wildschiodtz, G., & Tallgren, A. (1993). Head posture in obstructive sleep apnoea. European Orthodontic Society, 15, 107–114.
Timoshkin, E. M., & Sandhouse, M. (2008). Retrospective study of cranial strain pattern prevalence in a healthy population. The Journal of the American Osteopathic Association, 108(January), 652–656.
Tow, J., Boyd, K., Lynch, B., Jacobson, H., Buckley, S., Jaminet, P., & Masterjohn, C. (2014). Tongue-tie, Epigenetics, and the Microbiome.
Uhlig, S. E., Marchesi, L. M., Duarte, H., & Araújo, M. T. M. (2015). Association between respiratory and postural adaptations and self-perception of school-aged children with mouth breathing in relation to their quality of life. Brazilian Journal of Physical Therapy, 19(3), 201–210.
van der Put, N. M. J., Gabreëls, F., Stevens, E. M. B., Smeitink, J. A. M., Trijbels, F. J. M., Eskes, T. K. A. B., … Blom, H. J. (1998). A Second Common Mutation in the Methylenetetrahydrofolate Reductase Gene: An Additional Risk Factor for Neural-Tube Defects? The American Journal of Human Genetics, 62(5), 1044–1051. http://doi.org/10.1086/301825
Wilcken, B., Bamforth, F., Li, Z., Zhu, H., Ritvanen, A., Redlund, M., … Botto, L. D. (2003). Geographical and ethnic variation of the 677C>T allele of 5,10 methylenetetrahydrofolate reductase (MTHFR): findings from over 7000 newborns from 16 areas world wide. Journal of Medical Genetics, 40, 619–625.
Yang, B., Liu, Y., Li, Y., Fan, S., Zhi, X., Lu, X., … Sun, G. (2013). Geographical Distribution of MTHFR C677T, A1298C and MTRR A66G Gene Polymorphisms in China: Findings from 15357 Adults of Han Nationality. PLoS ONE, 8(3). http://doi.org/10.1371/journal.pone.0057917
Yeol, H., Jong, K., Jeong, I., Jung, H. D., Sohn, H., Duk, S., … Yun, S. (2013). Nasal Obstruction and Palate-Tongue Position on Sleep-Disordered Breathing. Clinical and Experimental Otohinolaryngology, 6(4), 226–230.
This content is being provided for informational purposes only and is not a substitute for medical advice.
Please consult your medical doctor or professional if you have medical concerns.
©️ 2022 Resonate Health. This video may not be duplicated, copied or shared unless authorized.